And MIT group of researchers led by Professor Dimitris Bertsimas built website tools allowing anybody to access the following information:
- 130+ international Covid-19 clinical studies, aggregated into a single dataset
- Insights - key characteristics of COVID-19 patients in an interactive summary
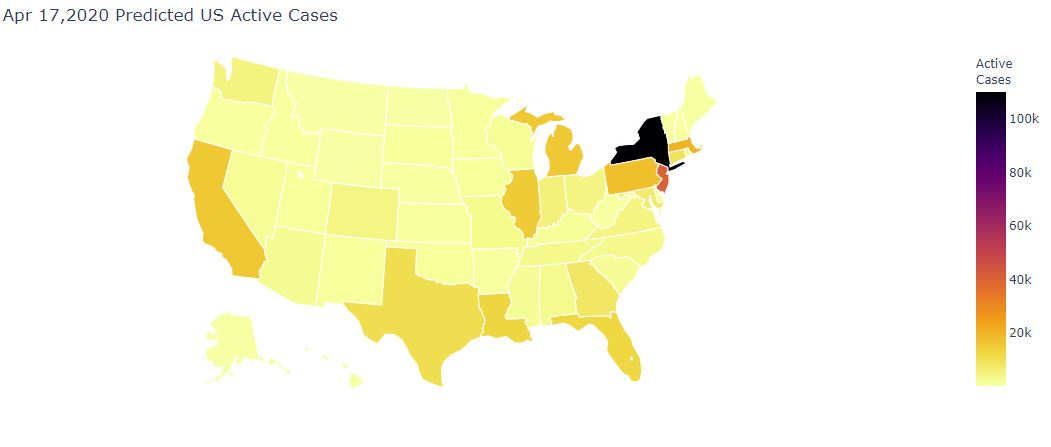
- Case Predictions - DELPHI epidemiological predictions of COVID-19 infections, hospital stays, and mortalities by location
- Ventilator Allocation - leveraging delays between state peaks to optimally re-use ventilators
- Risk calculator - personalized calculator predicting mortality given hospitalization.
A view of the analytics tools:

These tools can be accessed here.
These tools, for example, predict the following map of active cases on April 17th 2020 (today):
The COVID-19 pandemic is raising critical questions regarding the dynamics of the disease, its risk factors, and the best approach to address it in healthcare systems. MIT Sloan School of Management Prof. Dimitris Bertsimas and nearly two dozen doctoral students are using machine learning and optimization to find answers. Their effort is summarized in the COVIDanalytics platform where their models are generating accurate real-time insight into the pandemic. The group is focusing on four main directions; predicting disease progression, optimizing resource allocation, uncovering clinically important insights, and assisting in the development of COVID-19 testing.
“The backbone for each of these analytics projects is data, which we’ve extracted from public registries, clinical Electronic Health Records, as well as over 120 research papers that we compiled in a new database. We’re testing our models against incoming data to determine if it makes good predictions, and we continue to add new data and use machine-learning to make the models more accurate,” says Bertsimas.
The first project addresses dilemmas at the front line, such as the need for more supplies and equipment. Protective gear must go to healthcare workers and ventilators to critically ill patients. The researchers developed an epidemiological model to track the progression of COVID-19 in a community, so hospitals can predict surges and determine how to allocate resources.
The team quickly realized that the dynamics of the pandemic differ from one state to another, creating opportunities to mitigate shortages by pooling some of the ventilator supply across states. Thus, they employed optimization to see how ventilators could be shared among the states and created an interactive application that can help both the federal and state governments.
“Different regions will hit their peak number of cases at different times, meaning their need for supplies will fluctuate over the course of weeks. This model could be helpful in shaping future public policy,” notes Bertsimas.
Recently, the researchers connected with long-time collaborators at Hartford HealthCare to deploy the model, helping the network of seven campuses to assess their needs. Coupling county level data with the patient records, they are rethinking the way resources are allocated across the different clinics to minimize potential shortages.
The third project focuses on building a mortality and disease progression calculator to predict whether someone has the virus, and whether they need hospitalization or even more intensive care. He points out that current advice for patients is “at best based on age, and perhaps some symptoms.” As data about individual patients is limited, their model uses machine learning based on symptoms, demographics, comorbidities, lab test results as well as a simulation model to generate patient data. Data from new studies is continually added to the model as it becomes available.
“We started with data published in Wuhan, Italy, and the U.S., including infection and death rate as well as data coming from patients in the ICU and the effects of social isolation. We enriched them with clinical records from a major hospital in Lombardy which was severely impacted by the spread of the virus. Through that process, we created a new model that is quite accurate. Its power comes from its ability to learn from the data”, says Bertsimas.
“By probing the severity of the disease in a patient, it can actually guide clinicians in congested areas in a much better way,” says Bertsimas.
Their fourth project involves creating a convenient test for COVID-19. Using data from about 100 samples from Morocco, the group is using machine-learning to augment a test previously designed at the Mohammed VI Polytechnic University to come up with more precise results. The model can accurately detect the virus in patients around 90% of the time, while false positives are low.
The team is currently working on expanding the epidemiological model to a global scale, creating more accurate and informed clinical risk calculators, and identifying potential ways that would allow us to go back to normality.
“We have released all our source code and made the public database available for other people too. We will continue do our own analysis, but if other people have better ideas, we welcome them,” says Bertsimas.
Note: This work represents a collaborative effort with Hartford HealthCare and ASST Cremona which have been providing us with data and support through the model creation process.
]]>
























